
Why Everyone Is Talking About AI Diagnostic Tool Cartilage Damage 2026
A radiologist scoring knee osteoarthritis by hand still does what clinicians have done for decades: eyeball an MRI slice-by-slice and grade cartilage loss against a mental rubric. As a result, it doesn’t scale. Worse, it often misses damage that shows up years before a plain X-ray would catch anything.
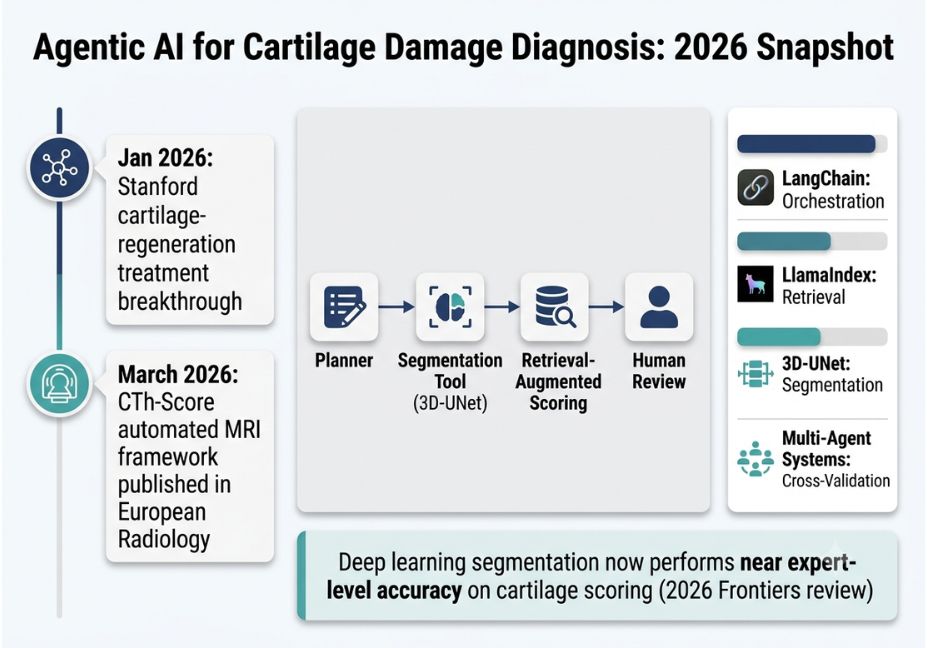
That’s starting to change. In March 2026, researchers publishing in European Radiology introduced an automated framework the CTh-Score that converts MRI scans into high-resolution cartilage thickness maps using a 3D-UNet segmentation model. According to the study, it matched expert-level reproducibility across large datasets from the Osteoarthritis Initiative. That’s a strong diagnostic model. However, on its own, it is not an agent.
So what’s the difference between an AI agent for cartilage damage diagnosis and a standalone diagnostic model? For readers building agentic AI systems, the more interesting story isn’t the scoring algorithm itself it’s the orchestration layer wrapped around it: the planner that decides which tool to call, the retrieval step that grounds a finding in prior imaging, and the report-generation step that hands a structured output to a human reviewer. In other words, this article breaks down how to build an agentic medical imaging pipeline, using cartilage-damage diagnosis as the worked example.
Quick answer: An AI agent diagnoses cartilage damage by orchestrating a segmentation model that maps MRI thickness, grounding that output with retrieval-augmented generation against reference scoring data, and routing the final structured finding to a human reviewer not by predicting a score in a single step.
What Is an Agentic Diagnostic Pipeline?
An agentic diagnostic pipeline differs from a standalone diagnostic model in one key way: it doesn’t just output a prediction it decides what to do next. Specifically, a segmentation model like the one behind CTh-Score produces a thickness map. Then an agent wrapping that model decides whether the map warrants a follow-up tool call: comparing against a prior scan, pulling relevant literature, or flagging the case for a second-opinion agent.
For example, GitHub’s Awesome-AI-Agents-for-Healthcare registry tracks dozens of these systems, including tool-using agents built specifically for stepwise interpretation of imaging studies. That registry is worth bookmarking if you’re prototyping an agentic AI workflow for medical imaging it’s updated with new arXiv preprints monthly. Of course, any pipeline headed toward clinical use also has to account for regulatory frameworks like the FDA’s software-as-a-medical-device pathway or the EU MDR, which is a separate consideration from the architecture itself but shapes how much autonomy the agent is ultimately allowed.
How Does an Agentic Cartilage-Diagnosis Pipeline Work?
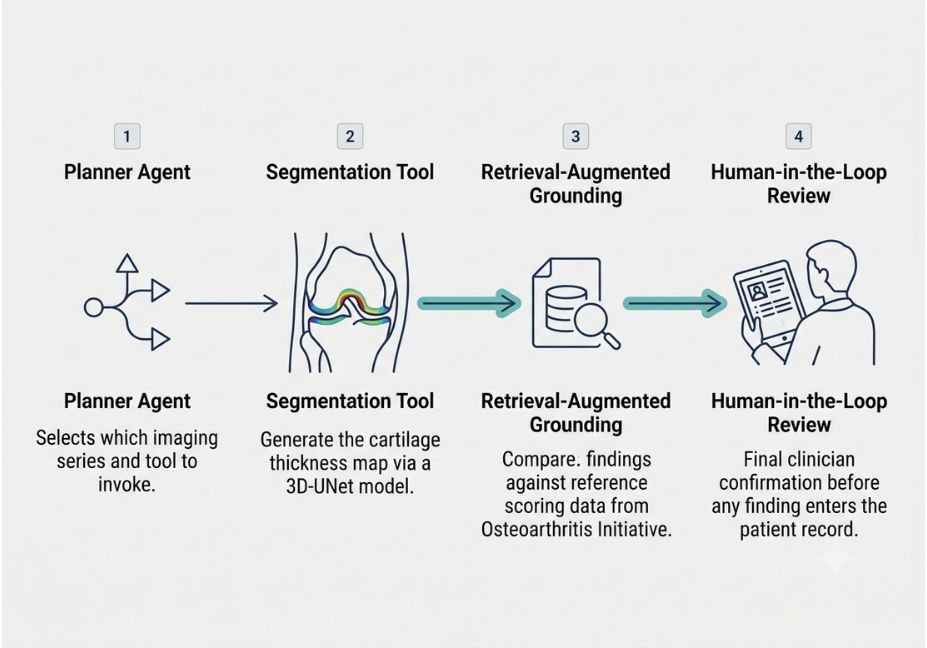
To understand how an agentic AI medical imaging pipeline actually works, break it into four stages:
- Planner an LLM decides which imaging series to analyze and which tool to invoke (segmentation, prior-scan retrieval, or literature search).
- Tool-use loop the agent calls a segmentation model (e.g., a 3D-UNet) to generate the thickness or defect map, following an architecture that combines tool use, explanation, and iterative analysis rather than a single forward pass.
- Retrieval-augmented scoring retrieval-augmented generation pulls comparable prior cases or published scoring thresholds so the agent’s output is grounded rather than freely generated.
- Report + human-in-the-loop review the agent drafts a structured finding, and a clinician confirms or overrides it before it enters the record.
Pro Tip: If you’re prototyping this kind of loop, model your planner on a ReAct-style tool-use loop LangChain’s agent documentation is the fastest way to see the pattern implemented, though it’s not medical-specific out of the box. (For a deeper walkthrough of the ReAct pattern itself, see our companion guide on tool-use loops on agentiveaiagents.com.)
Meanwhile, Did You Know? Deep learning segmentation systems are already performing close to expert level on cartilage segmentation and severity classification tasks, according to a 2026 review in Frontiers. That’s precisely why the interesting engineering problem has shifted from “can the model segment cartilage accurately” to “how do we orchestrate that model safely.”
Real-World Research Behind the 2026 Breakthrough
A few 2026 papers show where this is actually headed, not just where it could go:
- CTh-Score (Eur Radiol, March 2026) automatic MRI-to-thickness-map framework, with strong reproducibility for longitudinal monitoring.
- RadAgent a tool-using agent for stepwise chest CT interpretation, illustrating the same planner/tool-call pattern applied outside orthopedics.
- MedSAM-Agent interactive medical image segmentation via multi-turn agentic reinforcement learning, relevant to any pipeline that needs to refine a segmentation mask iteratively rather than accept the first pass.
- Separately, Stanford Medicine researchers found a treatment that can reverse cartilage loss and even prevent arthritis after knee injury by blocking an aging-linked protein a treatment breakthrough, not a diagnostic one, but it changes what a diagnostic agent’s output should trigger downstream (early intervention vs. monitoring).
Best Tools and Frameworks for Building This Kind of Agent
| Framework | Role in the pipeline | Notes |
|---|---|---|
| LangChain | Planner / tool-orchestration layer | General-purpose; needs a medical tool wrapper |
| LlamaIndex | Retrieval layer over prior scans/literature | Good fit for grounding scores in published thresholds |
| 3D-UNet (custom) | Segmentation tool | Domain-specific, trained on datasets like the Osteoarthritis Initiative |
| Multi-agent frameworks (MDAgents-style) | Cross-validation / second opinion | Adds a moderator agent that reconciles disagreeing findings |
Architect’s Note: Don’t let the planner call the segmentation model directly into a final report. Insert a retrieval step in between grounding the raw segmentation output against known scoring thresholds is what separates a defensible finding from a hallucinated one.
Step-by-Step: Implementing a Minimal Version
- Wrap your segmentation model (e.g., a 3D-UNet checkpoint) as a callable tool with a defined input/output schema.
- Give your orchestration agent a system prompt that forces a plan-then-act loop rather than a single-shot answer.
- Add a retrieval step pulling from a small corpus of prior cases or published scoring papers.
- Require the agent to output a structured object (finding, confidence, supporting citation) rather than free text.
- Route every output through a human reviewer before anything touches a patient record no exceptions.
def diagnose_cartilage(mri_series):
plan = planner_agent.plan(mri_series)
if plan.tool == "segment":
thickness_map = segmentation_tool.run(mri_series)
grounded = retriever.ground(thickness_map, corpus="oai_reference_scores")
return report_agent.draft(thickness_map, grounded)
return plan.fallback()Common Mistakes and How to Avoid Them
- Treating the segmentation model as the whole system. The model scores an image; the agent decides what that score means in context. Conflating the two leads to overconfident single-model deployments.
- Skipping retrieval grounding. Without it, an agent can generate a plausible-sounding severity grade that no reference dataset actually supports a known failure mode in this space, as agentic AI can reduce hallucination rates in radiology workflows when retrieval-augmented generation grounds responses in verified literature, though these methods remain computationally demanding and lack full clinical validation.
- No human-in-the-loop step. Every credible system in this space, including the research prototypes above, keeps a clinician in the final decision loop. Ultimately, that’s the difference between a research demo and a deployable clinical tool.
What Developers Are Saying
Discussion threads in orchestration-framework communities and in PubMed-indexed radiology-informatics journals keep circling back to the same tension: multi-agent medical pipelines improve accuracy on paper, but latency and compute cost stack up fast once you add a moderator agent for cross-validation. Consequently, that trade-off between accuracy and cost is the recurring theme in the actively maintained agentic-healthcare research registry on GitHub, where new preprints on this exact bottleneck appear most months.
FAQ People Also Ask
How do AI agents diagnose cartilage damage?
They don’t diagnose alone an agent orchestrates a segmentation model to map cartilage thickness from MRI, retrieves comparable reference data to ground the finding, and drafts a structured report for a clinician to confirm.
What is a multi-agent radiology system?
It’s a pipeline where separate agents handle distinct roles segmentation, retrieval, moderation and a coordinating agent reconciles their outputs, rather than relying on one model’s single prediction.
Can agentic AI replace a radiologist for cartilage scoring?
Not currently. Research systems keep a human reviewer in the loop specifically because grounding and hallucination risks remain unresolved at full clinical scale.
What’s the difference between a diagnostic AI model and an AI agent?
A diagnostic model produces a single prediction from an input. An agent decides which tools to call, in what order, and how to act on the results the model is one component inside it.
How do agentic systems avoid hallucinating imaging findings?
Primarily through retrieval-augmented generation, which grounds a generated finding in verified reference data or literature rather than letting the model generate a score unconstrained.
Conclusion
The 2026 cartilage-diagnosis breakthrough isn’t really about a better segmentation model the CTh-Score framework already handles that well. The more relevant shift for AI-agent builders is architectural: wrapping that model in a planner, a retrieval step, and a human-reviewed report loop turns a single prediction into a defensible clinical workflow. The same pattern plan, call a tool, ground the result, hand off for review shows up across nearly every serious agentic medical-imaging system published this year. Bookmark this guide and explore more agentic-workflow breakdowns at agentiveaiagents.com.





